
In surgery, the term «augmentation» is used for a specific type of intervention, for example, hardening (building) the skeleton of an organ. We will talk about the empowerment of biological vision at the expense of implants.
You can not just take out a piece of tissue from the eye, as during laser correction, but also insert something new there. For example, an implant that allows you to see at night. Or DVR. Or — what is being done now — just an internal contact lens made from a biocompatible polymer.
Therefore, when you read about new opportunities for contact lenses, remember — all this can be built into a person. Of the most promising technologies — transfer images from your eyes to a computer and vice versa. If you are lucky, in 10 years you will be able to search for a given word in a paper book, as you are now looking for on a web page.
But let's still go back to the real world and talk about phakic lisch, corrective vision for those who can not help the laser.
What are phakic lenses
Phakic lenses are intraocular lenses that are implanted in the eye with the presence of its own lens. To implant such a lens, it is not necessary to remove anything from the eye. It is simply the addition of a certain optical corrective device inside. Lenses can be of different designs. The first implants of this kind were created in the 60s of the last century, the first implantation was performed by Dr. Benedetto in Rome. The lens was made of polymethyl methacrylate (PPMA), a thermoplastic transparent plastic, placed in the anterior chamber of the eye and fixed in the angle of the anterior chamber. The early postoperative results were excellent, but later postoperative complications later arose, so the operation lost its popularity. Until the 80s of the twentieth century, it was forgotten until it was revived in Russia and Western Europe.
The first phakic lenses were just an experience to correct myopia. However, when you have a technology that allows you to correct optics by adding something rather than removing it, you are immediately tempted to add a little more ability to your eye than nature has to do.
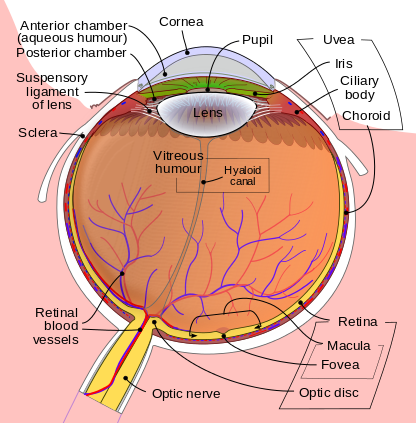
The anterior chamber in the figure above is the space between the cornea and the iris (above the lens, labeled Lens), it is filled with a clear liquid, there is relatively much space. The back camera is a narrow space from the bottom of the iris to the lens, there is significantly less space.
The difficulty is that:
- They increase the volume, that is, they must be in such a place so as not to damage the structures nearby and not to limit the circulation of the intraocular fluid.
- They should be stably fixed in the eye.
- They must be inert even after decades.
- And finally, they must correctly correct their vision, causing a minimal amount of optical side effects.

Phakic lenses are always in front of the lens in the anterior or posterior chamber of the eye. In the first case, they either touch the angle of the anterior chamber with their legs, or cling with “claws” to the iris. In the second case, they hide under the iris, swimming between it and the lens.
Both types have advantages and disadvantages. About irreversible complications — a little later. While we are interested in the fact that in both cases there is no contact with the lens of the eye, and the intraocular fluid circulates freely. Complications after implantation of a phakic IOL are caused by direct contact of the body or supporting elements of the IOL as a result of improper geometry or fastening.
Indications for IOL
- High degrees of myopia, not amenable to laser correction.
- High degrees of farsightedness, similarly — given that the laser correction is «asymmetrical», in the sense that the threshold for myopia is usually about -10, then for myopia — about +4, less often +6. Lenses maximally correct from +15 to -30 diopters and astigmatism up to 8 diopters (depending on the structure of the patient's eye).
- If the patient has a thin cornea that does not allow the evacuation of a sufficient amount of tissue for laser correction.
- Keratoectasia, i.e. corneal protrusion (keratoconus) — only for optical purposes.
- Presbyopia or age-sightedness.
Contraindications: too small camera to install the lens — anterior or posterior, glaucoma (increased intraocular pressure), a number of diseases of the cornea, lens, retina and vitreous body. Also installing an IOL may interfere with previously performed eye surgery. With a significant clouding of the natural lens, the violation of its ligament apparatus or its displacement, as a rule, an operation is needed to replace your own lens with an artificial one. Therefore, instead of implanting a phakic IOL, another method of treatment is used — the removal of one’s own lens with opacities and the implantation of an intraocular lens with suitable refractive parameters in place of one’s own lens.
When are phakic lenses put in?
Adding something to a healthy eye for no reason is superfluous. Therefore, phakic lenses are used today where it is impossible to solve the problem by other means. If a patient under 40 says “I want to take the glasses off”, the variant of one type of laser vision correction is first considered. We estimate the thickness, geometry, topography of the anterior and posterior surfaces of the cornea, its stability. And if there are no contraindications — laser correction is offered. First is the easiest way. Secondly — it is cheaper. Thirdly, it is not a penetrating type of surgery. That is, with the observance of technology, all risks are minimized. And, finally, a very high accuracy of the method, a very high quality of vision. And this is also the fastest way. And psychologically simple, of course.
In cases where laser correction cannot be performed due to the state of the cornea or high ametropia, the question arises about the possibility of implantation of a phakic IOL.
What result can I expect after implantation of a phakic lens?
The patient can rely on the visual acuity that he has with corrective glasses or contact lenses. Let me remind you that often we are talking about people with very large optical and medical problems. For example, high myopia, high farsightedness and high astigmatism are often accompanied by problems with retina or amblyopia (“lazy eye”). In these cases, before surgery, vision with correction in them does not reach 100%, then even after surgery it will not become 100%. We perform an operation to save the patient from glasses, and postoperative vision depends on the resolution of the retina in each case.
The quality of vision after implantation of a phakic IOL is the same as after laser vision correction.
By the way, I am often asked if people live with very great myopia, say -20 diopters. Such a view in ordinary life is often enough to pretty well navigate in space. If high myopia is found in childhood, then visit special kindergartens. Very often there are patients who with their -20 do not use glasses at all! Read «nose» — that is, Well, very, very closely placing the text, they work where there is no need for high visual functions, sometimes they wear high diopter contact lenses. One of the patients almost never used glasses, was engaged in physical labor. Of course, with such large «minuses», as a rule, problems are not only in the optics of the eye — various retinal complications are often revealed, cataracts — in general, any cocktail is possible.
If there are problems on the retina, or in the optic nerve, or in the cerebral cortex, the picture will fail and the vision will be low. It may happen that a person sees 2-3% of the norm, and after installing the lens will see 10-20% — this is detected in advance during the diagnosis. However, even this increase is very significant, since we estimate visual acuity not in decimal, but on a logarithmic scale — that is, the difference in visual acuity between the first and second lines is much more significant than between the ninth and tenth.
The following myth is related to the fact that before delivery it is impossible to make a correction.In fact, this is not the case; only the period of pregnancy and nursing is a contraindication. Childbirth can affect the retina if it has tears or detachment. Other parts of the eye are not injured during childbirth. Childbirth is the normal physiological condition of a woman. Eyes while working exactly as they should. If there are phakic lenses in the eyes or laser correction with the LASIK / FLEX, PRK or SMILE methods, there will be no problems.
And the last myth — after the correction, physical loads are excluded.Often, not very knowledgeable ophthalmologists tell patients: “You cannot lift anything, how is it that the lens is inside the eye, it will be torn away from you!”. Also not true, nothing special will be during exercise. In the 60s, yes, cuts and lenses were such that it was better not to sneeze once again. Today everything is much more technological and reliable. In general, phakic lenses are, most often, the choice of those who have contraindications to laser correction.
How fast is the phakic lens and what is the quality of vision?
Given that implantation of phakic lysna is a more invasive operation than laser correction by any of the methods, excellent vision quality is achieved on the same day. Moreover, as a rule, at the boundaries of indications (with vision -10) when comparing options with laser correction or installing a lens, the lenses give a better quality of vision. More patients are very surprised that nothing stings, does not prick. The patient immediately sees perfectly, almost rising from the operating table. This is a very fast and effective way of correction, just people know very little about it. And in Russia rarely.
What about Russian phakic lenses?
The Russian technology branch (lenses MNTK) vigorously developed for quite a long time. After Russian ophthalmologists met with complications after using lenses with fixation in the CPC, the institute under the guidance of S.N. Fedorov developed a new lens model, “mushrooms”, which was used from 1986 to 1990 in Russia. This model was different way of attaching the lens to the pupil. The main advantage was that it avoided contact of the lens with the endothelium. More than 100 lenses were implanted with a good result. This was the beginning of the era of phakic correction with lenses fixed in the back of the camera. The reference part of the lens was placed in the back of the camera, and the optical part remained in the front, so the lens was fixed pupil.
However, in the postoperative period, lens opacities and an increase in intraocular pressure were often observed, which required a change in the architecture of the lenses in order to avoid contact with the lens and cornea endothelium. In addition, inflammation and optical side effects often occurred at night.
Taking into account the experience of “lens-fungi”, Russian ophthalmologists have offered exclusively back-chamber phakic lenses made of a completely new silicone material, which was not toxic and had a higher refractive index. The configuration, parameters and fixation mechanism of these phakic lenses differed significantly from the “lens-fungi”. Negative posterior chamber lenses were created to correct a high degree of myopia of more than -10.0 diopters. This lens has become the prototype of all the posterior chamber lenses currently on the market.
Now, however, European-made lenses, although more expensive, are much better. The reason is very prosaic: significantly less chance of irreversible side effects in the long run.
Operation process for phakic posterior chamber lens
Premedication with anesthetics (for example, with drops of alkaine, as with laser correction), the pupil expands to the maximum. The incision is made from 2.5 to 3.5 millimeters on the cornea, this is a tunnel for access to the area between the iris and the lens. A special viscous solution is introduced into the eye to maintain the volume of the eye. Through the incision made, a folded lens is inserted, which then straightens, and its legs are tucked under the iris. Pupil narrows as much as possible. Pre- or intraoperatively, 1-2 tiny holes are made in the iris for proper circulation of fluid inside the eye. Then the viscous solution is washed out. The whole operation takes from 10-15 minutes. In the first operations, rigid lenses were historically used, and, accordingly, much larger incisions had to be made for access. In this case, they were placed in the anterior chamber of the eye or clung to the iris. Since then, the technology of manufacturing lenses changed many times. Today, most often used soft lenses made of silicone with a biotic base (pork collagen) — they best take root. The “fixings” of the lenses also evolved for quite a long time — for example, iridofixation lenses cling to the iris with “claws”. In more detail about the features of the operation, I will tell you later, there are some nuances.
These are the lenses
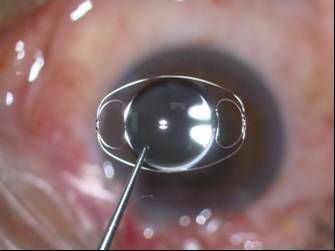
Anterior chamber phakic IOL with fixation in the corner of the anterior chamber:

She after implantation
Anterior chamber with fixation «claws» for the iris:
Posterior chamber phakic IOL PRL:


Posterior chamber phakic IOL ICL:



Variants of lenses of the Russian manufacturer NEP. Microsurgery of the Eye. S.N. Fedorova from collagen copolymer:
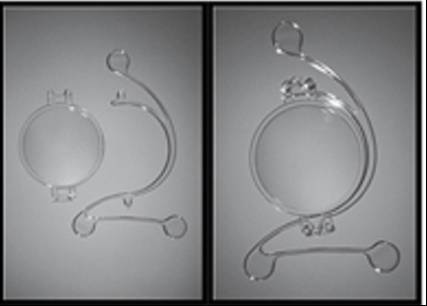
This is a completely unique copy of the “collapsible” fakichnoy IOL Duett lens — as needed it can change the optical part.
Yes, phakic lenses can be replaced if necessary. An operation similar to installing a lens is carried out, only after providing access, the surgeon first removes the old lens, and then puts a new lens in its place or, in the case of a cataract, removes a cloudy lens and puts a model with implantation in a capsular bag.
Requirements for the surgeon
Phakic lenses are a product of individual manufacturing. In order to order a lens for the patient, the clinic should have sophisticated measuring devices, and the surgeon should have experience in implanting and calculating these lenses (best of all with thousands of cataract operations) perfectly representing the anatomy and physiology of the eye.
One of the methods of optical correction of the eye with keratoconus can also be a phakic lens. In such patients, optics often exceed myopia more than 10-12 diopters in combination with irregular astigmatism — they see very poorly without correction, usual soft contact lenses do not fit, and correction remains with hard contact lenses. To reduce the dependence on the lenses and increase the uncorrected visual acuity, a phakic IOL is implanted (keratoectasia is stabilized by cross-linking, then a phakic lens is placed). Accordingly, practice is needed in working with these operations.
There are cases when one eye is suitable for conventional laser correction (femtoLASIK or ReLEx SMILE), and the second requires intervention with a phakic IOL. The quality of vision at the same time is comparable in both eyes in the postoperative period, and rehabilitation is just as fast. So this is a great way for non-standard situations.
In terms of the number of operations in Russia, these are usually isolated cases of installing phakic lenses per month with hundreds or thousands of laser corrections. For example, I have the last year from 2 to 4 cases of phakic IOLs per month, and laser corrections from three hundred to one thousand per year.
Result
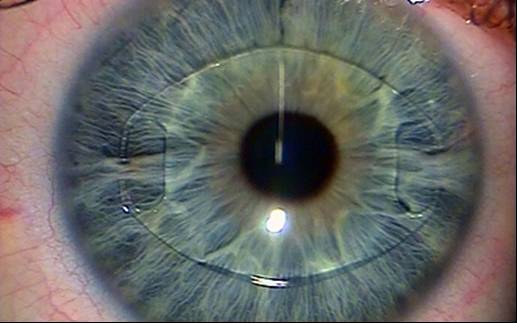
This is how the eye with a posterior chamber phakic lens looks like — the lens is visible only in a thin section of the microscope in front of its own lens:

This is an example of the implantation of a posterior chamber phakic lens after the expansion of the pupil:

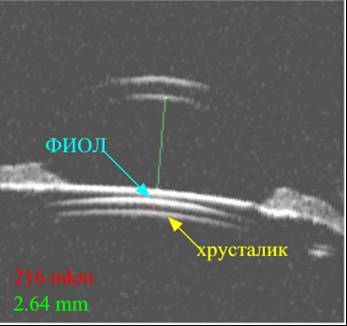
Ultrasound biomicroscopy of the eye with phakic posterior chamber IOL:
What can I put in addition to the usual phakic lens?
Here is an example of a contact lens containing a sensor and a device for receiving and transmitting information, as well as wireless charging:

The sourceк, it is needed to monitor glucose levels, a project for the International Federation of Diabetes.
The first experiments with «smart» lenses, a consequence. Here is the screen printing technology on these lenses. Here is another prototype. And there is a patent application from Google for the lens with limited focusing capability (US20160113760).
In 2012, Dr. Michel Makharbiz reported on how to take data from beetles' eyes -«AD Jadhav, I. Aimo, D. Cohen, P. Ledochowitsch, and MM Maharbiz, CYBORG EYES: MICROFABRICATED NEURAL INTERFACES IMPLANTED DURING THE DEVELOPMENT INSECT SENSORY ORGANS PRODUCE STABLE NEURORECORDINGS IN THE ADULT».
The point is that after 10 years instead of the usual phakic lenses made of copolymer, full-fledged computers will be installed in the eye.
Past posts about laser correction: Laser that cuts inside the cornea: ReLEx procedure at the physical level, FAQ about laser correction ReLEx SMILE: yes, in Russia there is, but no, in Russia there isn’t, A couple more unobvious things that you might not be told before laser vision correction.
